The Role of Mast Cells in Allergic and Inflammatory Processes
Copyright Algonot Health Sciences July 8, 2024
Almost 30% of people have allergies and many more have food intolerance,
while others are sensitive to multiple environmental and stress stimuli that can
affect numerous tissues/organs leading to a variety of symptoms that can be very
confusing and have be called “mystery symptoms.”
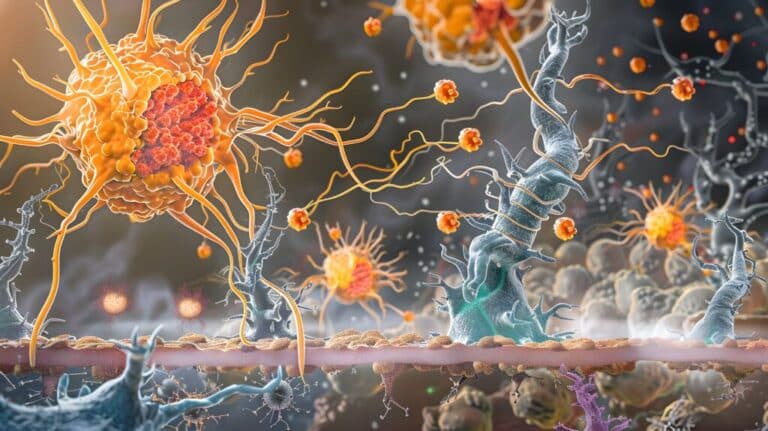
These symptoms are largely due to activation of a unique tissue immune cell, the
mast cell, (Fig. 1) that “orchestrates” the immune response of the body to a real
or perceived danger. Activation of mast cells is typically associated with allergic
reactions but is also critical for inflammatory processes.
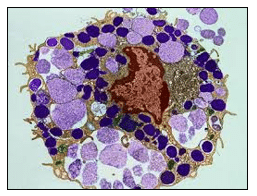
toluidine blue showing the state of degranulation during which the content
of most of its secretory granules is secreted (light violet) while the intact
granules are stained dark blue.
Mast cells are located close to blood vessels and neurons in all tissues,
especially those exposed to the outside world (e.g. eyes, nose, mouth, lungs,
skin and gastrointestinal tract), but also the brain (see discussion later). Mast
cells derive from the bone marrow, enter the blood as undifferentiated precursor
cells and “mature” in the tissues under the influence of local micro-environmental
factors. There, they can develop different phenotypes (mediators produced and
reactivity) and have typically been divided based on their secretory granule
content of proteolytic enzyme (proteases). Mucosal mast cells (MMC) contain
only the enzyme tryptase while connective tissue mast cells (CTMC) contain both
chymase and tryptase. Histamine is stored in the secretory granules of both
subtypes. Mast cell granules also store tissue remodeling enzymes, such as
carboxypeptidase A3 (CPA3) and matrix metalloproteinases (MMPs). However,
mast cell phenotypes may be modified depending on the triggers. All types of
mast cells synthesize, store and can release histamine.
In allergic reactions and in anaphylaxis, mast cells are triggered by allergens
bridging immunoglobulin ((IgE) bound to its specific receptors (FcεRI) on their
cell surface (Figure 2), but also positively charged molecules and drugs via
activation of a different receptor (MRGPRX2). When mast cells are triggered by
FcεRI or via MRGPRX2, there is rapid secretion, called degranulation by
exocytosis (Fig. 1) of many preformed molecules, stored in as many as 1000
secretory granules per cell, some of which are shown in the box on the lower
right-hand side of Figure 2.
Histamine and tryptase are the best known prestored molecules. In addition to
histamine, tryptase has been studied extensively because it is considered an
exclusive mast cell-associated mediator and is released during anaphylaxis and
systemic mastocytosis, as well as in some cases of mast cell activation.
Histamine is also released from basophils, which circulate in the blood. In many
cases of chronic itching (urticaria), mast cells are activated by IgG antibodies
against the FcεRI receptor.
Leukotrienes (involved in bronchoconstriction) and prostaglandins (involved in
pain) are also rapidly produced during mast cell stimulation. Histamine,
leukotrienes and prostaglandins are rapidly degraded and are seldom measured
in the blood; instead, their breakdown products (metabolites) are measured in
24-hour urine that has to be kept cold.
Theoharides TC, et al. N Engl J Med. 2015;373(2):163-72.
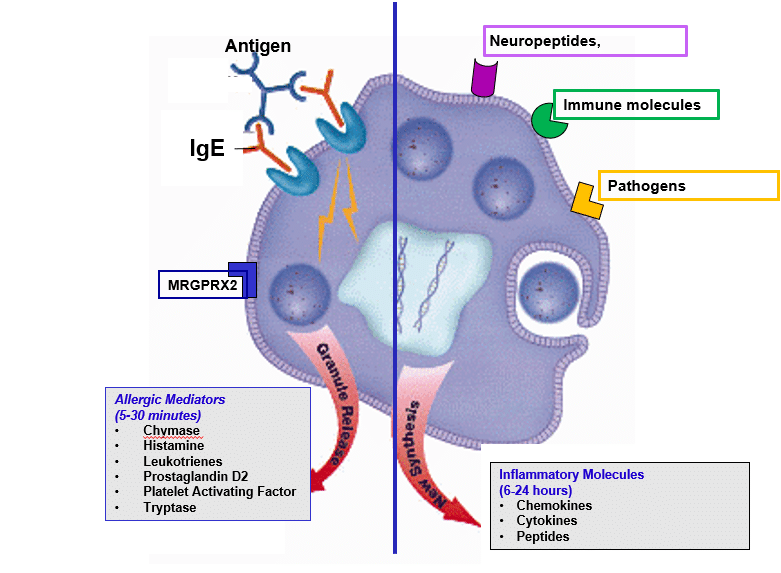
In addition to allergic stimulation, mast cells are stimulated by numerous non-
allergic triggers (Figure 2), especially neuropeptides released from nerves such
as corticotropin-releasing hormone (CRH) and substance P (SP), immune
molecules such as interleukins (IL-1β, IL-33) and pathogens such A bacteria,
fungi and viruses. Following stimulation by these non-allergic triggers, mast cells
synthesize new inflammatory mediators (some of which are shown in the box on
the lower right-hand side of Figure 2) that are released (right-hand side box of
Figure 2) without histamine and without degranulation (differential release).
Molecules such the cytokine IL-6 and vascular endothelial growth factor (VEGF)
may reflect non-allergic stimulation, edema and inflammation. By rapidly
releasing these mediators, mast cells actively interact with other cell types in their
surrounding environment and participate in the induction and/or propagation of
various allergic, inflammatory and immune responses. Depending on the trigger
and the different mediators released, mast cells can affect any and all organs of
the body including the brain, leading to very confusing, multisystem
symptomatology (Figure 3). In fact, affected individuals can often present with
symptoms mimicking many different overlapping diagnoses.
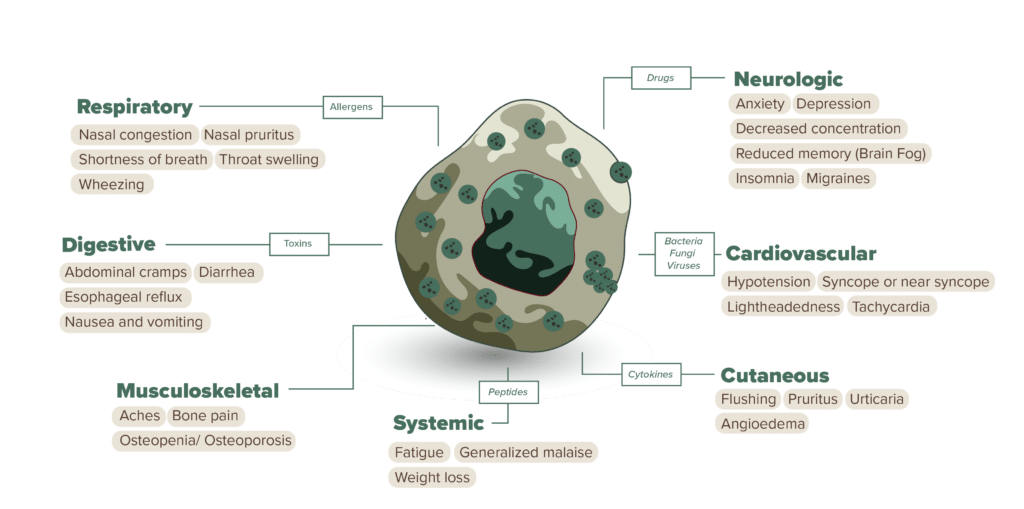
Diagrammatic representation of how mast cell activation by different
triggers may affect all organs in the body leading to different symptoms
that may resemble other medical conditions.
Theoharides TC, et al. Expert Rev Clin Immunol. 2023(6):639-654.
Mast cells communicate with neurons outside and inside the brain, especially in
the meninges, amygdala, hippocampus and hypothalamus, brain regions that
regulate behavior, memory and homeostasis, respectively. Mast cells are the
richest source of histamine in the brain. Brain mast cells had been termed the
“immune gate to the brain” (Figure 4) because they regulate permeability of the
protective protective blood-brain-barrier (BBB). Mast cell-derived vasodilatory
mediators (bradykinin, histamine, tryptase, VEGF) can disrupt the BBB, activate
the brain’s defenders, the microglia, leading to localized inflammation, oxidative stress, disrupted neuronal communication, neurodegeneration and cognitive
dysfunction, commonly known as “brain fog.”
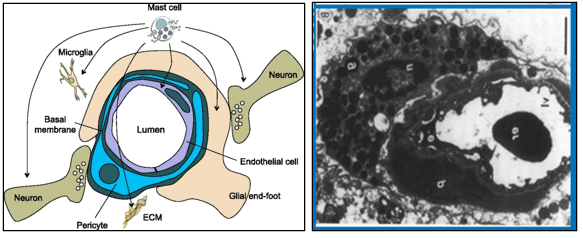
endothelial cells (violet) and the pericytes (blue) with one mast cells at the
top. (B) Electron micrograph of the BBB from the hypothalamus showing
the lumen of blood vessel with one erythrocyte (er) the endothelial cells (e),
the pericytes (p) and one mast cell at the left with numerous intact
secretory granules (g) embracing the blood vessel (magnification=30,000
diameters).
Theoharides TC. Life Sci. 1990;46(9):607-17.
Many large epidemiological studies have shown a statistically significant association between behavioral and cognitive problems in children, and allergic diseases that involve activation of mast cells. Mediators released from mast cells could be involved because they: (a) increase the permeability of the blood-brain barrier (BBB) and allow toxins to enter into the brain (b) stimulate microglia and release metalloproteinases , enzymes that damage the brain matrix and disrupt neuronal connectivity.
Mediators released from mast cells in the brain, as well as other substances entering the brain from a disrupted BBB can activate the brain’s defenders, the microglia, leading to localized inflammation, oxidative stress, disrupted neuronal communication, neurodegeneration and cognitive dysfunction, commonly known as “brain fog (Figure 5).
The effect of stress on mast cells has been well documented. Stress via release of corticotropin-releasing hormone (CRH) stimulates mast cells directly, but also increases their reactivity to many other triggers, especially peptides released from nerves such as nerve growth factor (NGF), neuropeptide Y (NPY) and substance P (SP). Such an increase in mast cell reactivity has been reported after major surgery, trauma or other severe stressor. Mast cells can also stimulate the brain defenders microglia and both release inflammatory molecules [histamine, IL-1beta, IL-6, IL-33, metalloproteinase-9 (MMP-9), TNFalpha, tryptase) that damage neurons. (Figure 5)
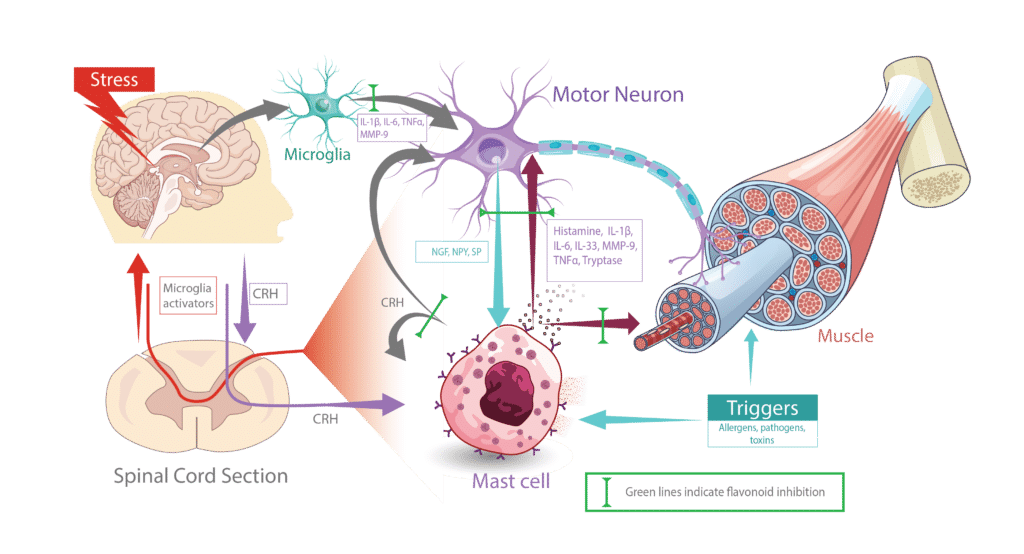
Theoharides TC, et al. Ann Allergy Asthma Immunol. 2024;132(4):440-454.
Many large epidemiological studies have shown a statistically significant association between behavioral and cognitive problems in children, and allergic diseases that involve activation of mast cells. Mediators released from mast cells could be involved because they: (a) increase the permeability of the blood-brain barrier (BBB) and allow toxins to enter into the brain (b) stimulate microglia and release metalloproteinases , enzymes that damage the brain matrix and disrupt neuronal connectivity.
Theoharides TC, et al. Transl Psychiatry. 2016;6(6):e844.
Such children improved with the use of NeuroProtek®, which also resulted in a significant decrease of serum levels of pro-inflammatory markers.
Theoharides TC. J Pers Med. 2021;11(9):860.
The incredible diversity of mast cell phenotypes and the ability of mast cells to
release hundreds of different mediators in response to allergic and nonallergic
triggers allows the mast cells to act as master immune regulators in the
pathophysiology of many different conditions (Figure 6).
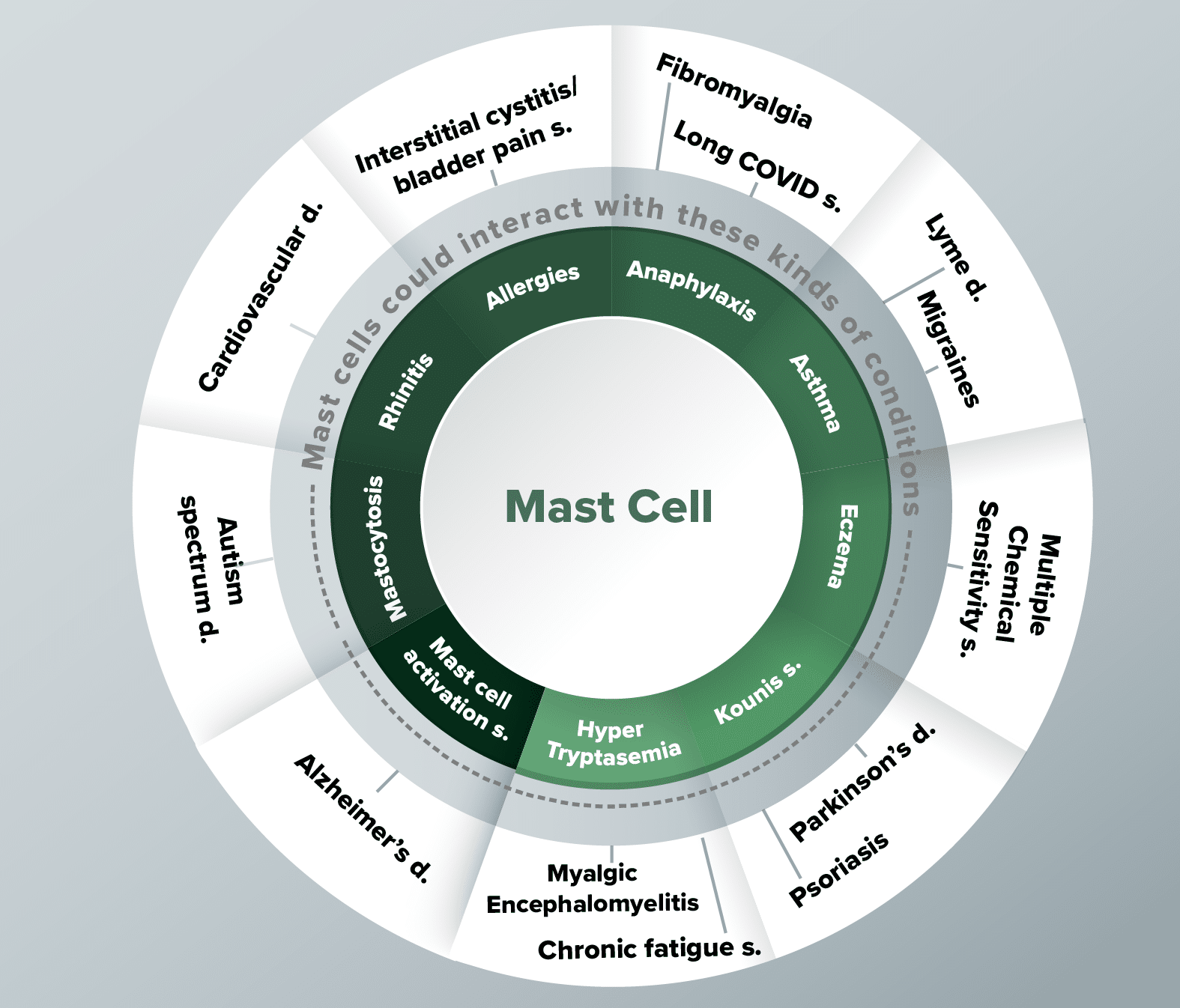
different conditions. The colored petals indicate strong evidence while the
clear petals indicate weaker associations.